The Endocannabinoid System: Here the Whole Time

Table of Contents
A system named after the plant that revealed it
The endocannabinoid system has an awkward name, and there is no point pretending otherwise. It is named for cannabis because cannabis is how we found it. In the 1960s, an Israeli researcher named Raphael Mechoulam isolated THC and CBD from the plant and asked the obvious next question: what, exactly, in the human body responds to these molecules? The answer turned out to be a regulatory system that almost no one had been looking for.
The first cannabinoid receptor — CB1 — was characterized in 19901. The second — CB2 — followed in 19932. Then came the molecules our bodies make to bind those receptors. Anandamide, named after the Sanskrit word for bliss, was identified in 19923. 2-arachidonoylglycerol — 2-AG — was characterized in 19954. By the late 1990s the picture was clear: humans have a built-in signaling network that uses cannabinoid-shaped molecules to regulate balance across nearly every tissue in the body.
This is what I want you to take from that history. The endocannabinoid system was not discovered because someone went looking for a master regulatory network. It was discovered backward — by chasing what cannabis does, scientists stumbled into a fundamental piece of human biology that had been there the whole time. Most of the textbooks women my age studied from didn't include it. Most of the doctors who trained women my age never learned it. That is not anyone's fault. It is just where the science was when the curriculum was written. The science has moved.
When I first started working with plant medicine for my own body, I had no idea any of this existed. Surgery saved my life — and I started looking for what would help me thrive without chemotherapy. Nobody mentioned cannabinoids. The ECS was barely a footnote in the literature my doctor was reading. Now it is one of the most-studied regulatory systems in human biology — and the convergence between what I was already doing with topicals and what the research now describes at the molecular level is one of the reasons Rockstar Blends exists.
What the endocannabinoid system actually does
The simplest accurate description is this: the ECS keeps things in range.
Your body runs on a continuous balancing act. Body temperature, blood pressure, blood sugar, sleep-wake cycles, immune response, pain perception, mood, appetite, fertility — every one of these has to stay within a livable range while everything around you constantly changes. Stress, food, sleep, season, infection, injury, hormone cycles, age. The biological term for the body's ongoing effort to hold itself in range against all of that is homeostasis. It is the most boring word in medical school and the most important word in your body.
The ECS is one of the body's primary instruments for maintaining homeostasis5. It does this with three components working together:
- Receptors embedded in cell membranes (CB1, CB2, and several others that respond to cannabinoid-shaped molecules)
- Endocannabinoids — molecules your body makes on demand, primarily anandamide and 2-AG
- Enzymes that build endocannabinoids when they're needed and break them back down when their work is done
The choreography matters more than the parts list. Endocannabinoids are not stored in advance the way some neurotransmitters are. They are synthesized on demand from lipid precursors in the cell membrane, released, allowed to do their job, and then enzymatically degraded so the signal does not run too long. This is one of the elegant features of the system — it is self-limiting by design6. Anandamide is broken down by an enzyme called FAAH (fatty acid amide hydrolase). 2-AG is broken down primarily by MAGL (monoacylglycerol lipase). Both enzymes are part of the system, not external to it.
When researchers in the 2000s started looking carefully at how endocannabinoid signaling works at synapses, they discovered something genuinely unusual. In most neural communication, the signal travels in one direction — the presynaptic neuron releases neurotransmitter, the postsynaptic neuron receives it. Endocannabinoids work in reverse. They are released from the postsynaptic neuron and travel back to the presynaptic side, where they bind CB1 receptors and quiet the original signal. This is called retrograde neurotransmission6. The body uses it to keep neural firing from running away with itself — a real-time braking system for excitatory signaling.
That braking function is part of why the ECS shows up in conversations about anxiety, pain, sleep, and inflammation. When the body needs to dial something back, the ECS is one of the systems it reaches for first.
"The endogenous cannabinoid system has significant roles in both health and disease. Drugs that mimic, augment, or block these endogenously released cannabinoids may have important therapeutic applications."
Pertwee RG · British Journal of Pharmacology · 20067
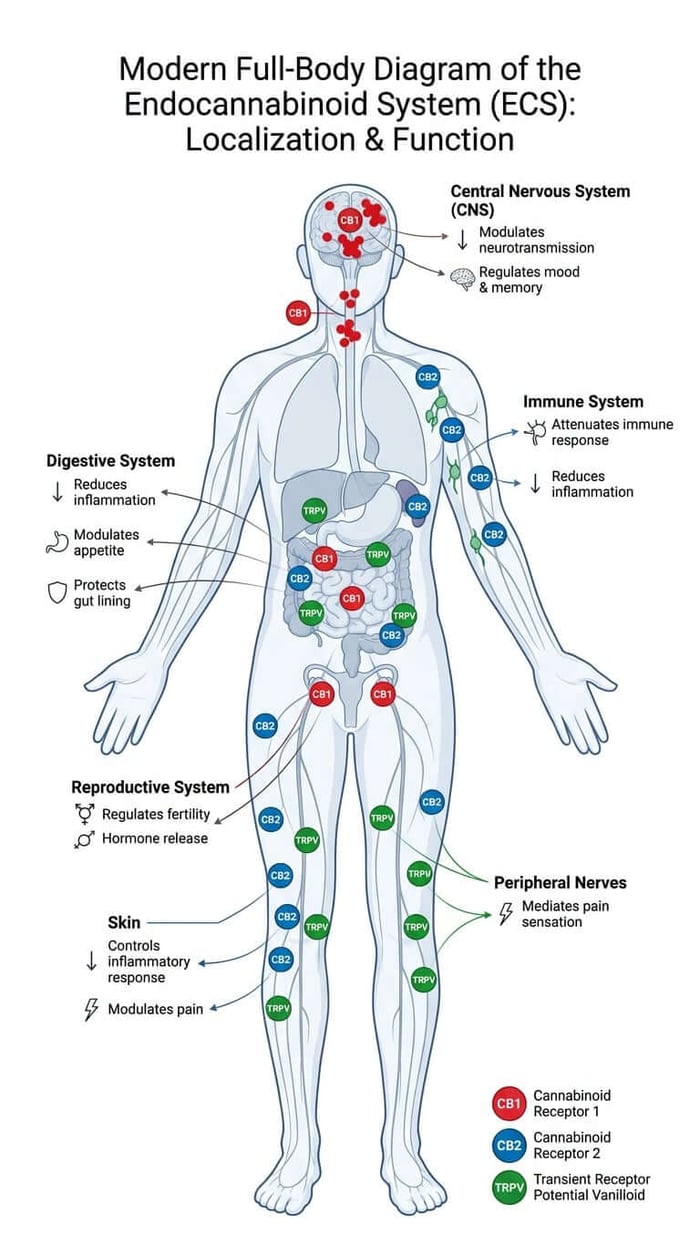
The receptors, and where they live in your body
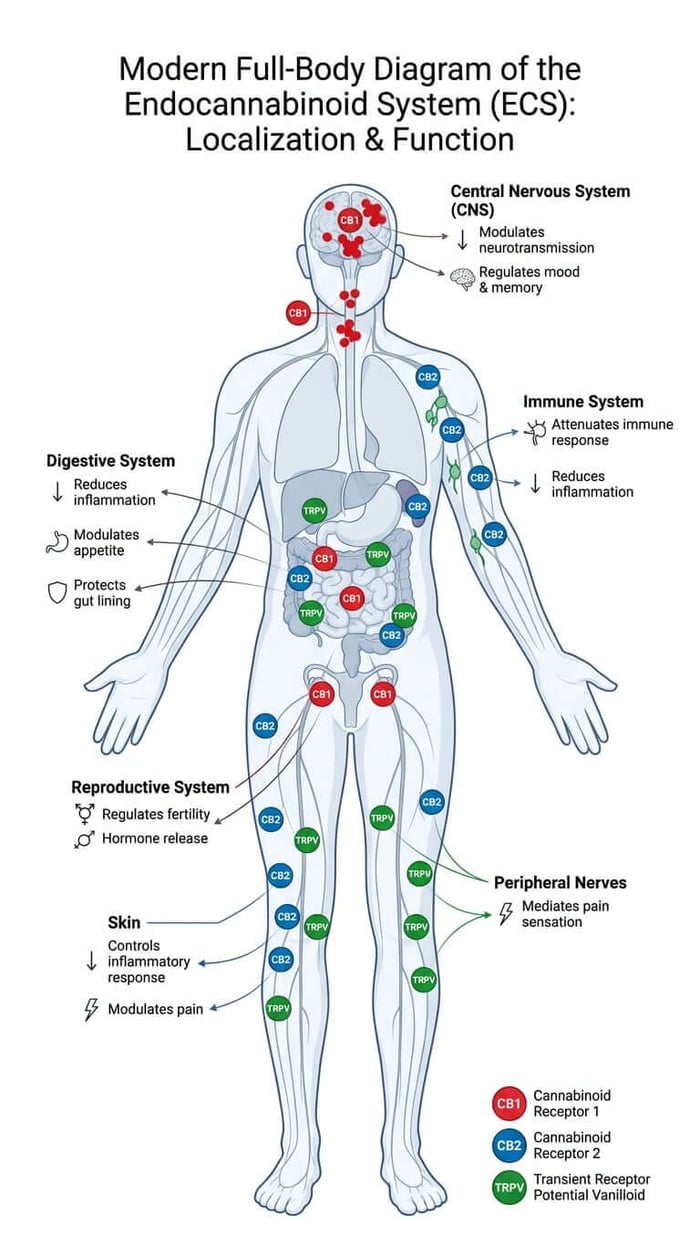
CB1 and CB2 are the two best-studied cannabinoid receptors, and they live in very different neighborhoods.
CB1 receptors are concentrated in the central nervous system — brain and spinal cord — with the densest expression in regions that handle memory, motor control, emotion, and reward1. They are one of the most abundant G-protein-coupled receptors in the brain. CB1 binds THC well, which is why THC produces the cognitive and mood effects it does. CB1 also binds anandamide and 2-AG — your body's own ligands for the receptor — at lower intensity and with more controlled release.
CB2 receptors are concentrated outside the central nervous system — primarily on immune cells, in lymphoid tissue, in the gut, and in the skin2. CB2 activation modulates inflammation, immune response, and pain perception at the peripheral level. CB2 has no significant psychoactive effects. It is the receptor most directly involved in inflammation control, and it is one of the reasons topical preparations applied to skin can do meaningful work without needing to cross the blood-brain barrier.
Both receptors share architecture and are part of the same family, but their signaling cascades are different and their distributions barely overlap. Think of CB1 as the central regulator and CB2 as the peripheral regulator — a useful simplification, even if biology resists clean lines.
And now the part where everyone gets it wrong. CBD — the compound most people associate with the wellness side of the cannabinoid conversation — has low direct binding affinity at CB1 and CB2 at the doses most people use8. It is a low-affinity, partially-active ligand at both, and can also act as a negative allosteric modulator at CB1. So how does CBD work?
The answer is that CBD acts through other receptors entirely. The most-studied of these are the TRP channels — transient receptor potential ion channels — which sit on cell membranes and respond to temperature, irritants, and certain plant compounds. Several TRP channels (TRPV1 in particular, but also TRPV2, TRPA1, and TRPM8) bind CBD with measurable affinity9. TRPV1 is the same receptor that responds to capsaicin in chili peppers. CBD also modulates serotonin receptors, adenosine signaling, and the enzyme FAAH — meaning it can raise your body's own anandamide levels by slowing the enzyme that breaks anandamide down10.
This is part of why "the ECS" is increasingly described in the literature as the endocannabinoidome — a broader interconnected network that includes the original CB1/CB2 receptors and a series of related receptors and signaling molecules that all use lipid-based messengers and overlap functionally with each other11. The simple two-receptor picture is correct but incomplete. The actual picture is bigger, messier, wired through more of the body, and more interesting than the textbooks have caught up to.
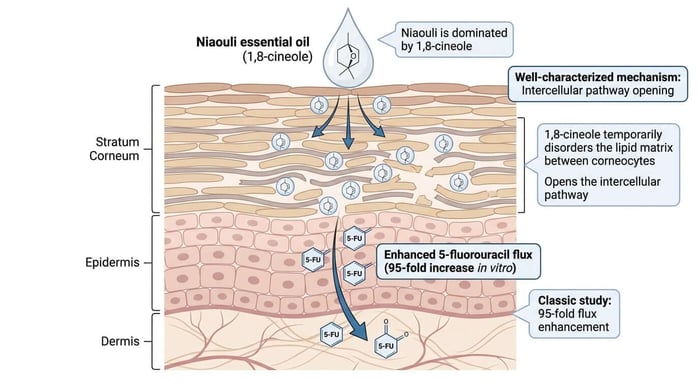
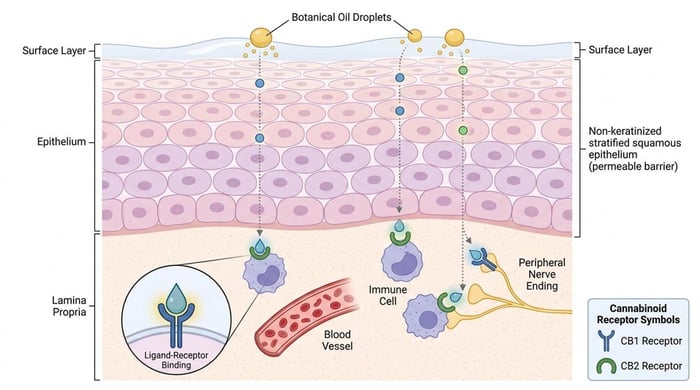
A practical note for women reading this: TRP channels are expressed across nearly every tissue type in the body9. The communication routes the ECS uses are not specialized hardware found only in your brain or your immune system. They are wired through nearly every tissue you have. That has implications for what topical preparations can reach — and it is part of why a roll-on applied to skin is a serious pharmacological delivery route, not a cosmetic one.
Why this matters more after 40
So why am I writing about a balance system for women in perimenopause and menopause specifically? Because estrogen and the endocannabinoid system are tightly coupled — and when estrogen declines, the ECS does not just keep running quietly in the background like it did at thirty-two.
Several lines of research now establish that 17β-estradiol — the principal form of estrogen during reproductive years — directly modulates the endocannabinoid system.
Estradiol stimulates the enzyme NAPE-PLD, which is the enzyme that builds anandamide12. Estradiol also inhibits FAAH, the enzyme that degrades anandamide. The net effect: when estrogen is high, anandamide tone tends to be high. When estrogen drops — across the menstrual cycle, across the perimenopausal transition, and into postmenopause — anandamide tone tends to drop with it. Estradiol also regulates CB1 expression in a region-specific way across the brain13, meaning the receptor density itself shifts with hormonal state.
The reproductive tissues themselves express ECS components throughout — ovary, uterus, fallopian tube, vaginal tissue, breast tissue all show CB1, CB2, and the enzymes that build and break down endocannabinoids14. Estrogen and the ECS regulate each other in a continuous feedback loop. When the loop loses its principal input — estrogen — the loop changes shape.
This is the bridge between I am not who I was a year ago and here is what is actually changing at the cellular level. The list of complaints — sleep that stopped working, mood that swings without warning, joints that hurt for no reason, skin that suddenly behaves like someone else's, the libido conversation nobody wants to have at the dinner table, brain fog you can feel in real time — overlaps almost completely with the list of systems the ECS regulates. That is not coincidence. It is the same system telling the same story from different angles.
And the data is starting to catch up to what women have been quietly figuring out on their own. A 2022 study published in Menopause found that 78.7% of peri- and postmenopausal women using medical cannabis reported using it specifically to target menopause symptoms15. That is not a clinical trial. It is a self-report survey, with all the limitations that implies. But it is a meaningful signal that women are reaching for cannabinoid support to address menopausal symptoms, ahead of the formal evidence base — and the mechanistic plausibility for why is real.
What the literature supports strongly
- The endocannabinoid system exists across nearly every body system and is one of the body's principal homeostatic regulators511
- CB1 receptors are densely expressed in the central nervous system; CB2 receptors are densely expressed in immune tissues, gut, and skin12
- Anandamide and 2-AG are synthesized on demand from membrane lipids and degraded by FAAH and MAGL respectively346
- CBD has low direct binding affinity at CB1 and CB2 and can act as a negative allosteric modulator at CB1; CBD's primary mechanisms involve TRP channels, FAAH inhibition, and serotonin receptor modulation8910
- Estradiol directly regulates anandamide synthesis (NAPE-PLD) and degradation (FAAH); the ECS and estrogen are mechanistically coupled1213
Supported as a class effect
- The endocannabinoidome model — that ECS-related signaling extends beyond CB1/CB2 into a wider network of receptors using shared lipid messengers11
- Phytocannabinoids and certain terpenes (β-caryophyllene as a selective CB2 agonist) engage the same receptor system the body uses for its own endocannabinoids
- Topical application can reach CB2 and TRP receptors in skin and peripheral tissue — mechanism is established for the receptor class
What would require a study we haven't run
- A clinical outcome specifically in menopausal women using a Rockstar Blends formulation
- A controlled trial of CBD, CBN, or phytocannabinoid blend versus placebo for any defined menopausal symptom
- A direct measurement of endocannabinoid tone before and after phytocannabinoid intervention in perimenopausal or menopausal women specifically
How phytocannabinoids enter this picture
Phytocannabinoids are plant-made compounds that interact with the same receptor systems the body uses for its own endocannabinoids. The cannabis plant produces over 100 of them. Many other plants also produce compounds that engage this system — copaiba, black pepper, hops, certain pine species, clove — though usually with fewer compounds and different proportions.
The four worth knowing by name:
- CBD (cannabidiol): The most-studied non-intoxicating cannabinoid. Engages TRP channels and modulates FAAH activity. Indirect ECS support rather than direct receptor binding8910.
- THC (tetrahydrocannabinol): Binds CB1 directly. Produces the cognitive and mood effects associated with cannabis. Federally regulated.
- CBN (cannabinol): Forms when THC oxidizes. Lower CB1 affinity than THC. Has emerged in human RCT data as relevant for sleep16.
- β-caryophyllene: A terpene rather than a classical cannabinoid, but a confirmed selective CB2 agonist17. Found in copaiba, black pepper, clove, and rosemary. One of the few CB2-active compounds you can encounter in foods and topicals.
A note on what "full-spectrum" actually means. A full-spectrum hemp extract is one that contains not just CBD but the accompanying cannabinoids and terpenes present in the source plant — the integrated phytochemical matrix. The working hypothesis in the field — sometimes called the entourage effect — is that this integrated matrix produces different effects than isolated CBD alone18. The hypothesis has directional support and is still being actively refined in the literature. It is not yet definitively settled, but the comparative evidence is real.
This is what I have been doing with Rockstar Blends. Every formula in the line is built around full-spectrum hemp paired with botanical extracts chosen for the compounds they bring to the receptor system — copaiba for β-caryophyllene, black pepper for both β-caryophyllene and penetration enhancement, frankincense for AKBA and incensole acetate, and others. The point is not to pick one molecule and load it. The point is to assemble a coherent topical preparation that engages the system the body already uses, applied where the receptors are densely present.
What the research has not yet answered
I want to be specific about this section because this is the part where Rockstar Blends sets its own standard.
We do not have a menopause-specific randomized controlled trial of any phytocannabinoid for any specific symptom endpoint. The closest adjacent evidence:
- The Bonn-Miller 2024 CBN sleep RCT (n=293) and the Kolobaric 2024 CBN sleep RCT (n=1,020) both show CBN at modest doses improves sleep without next-day grogginess1619. These were adult populations with sleep disturbance — not menopause-specific.
- A 2022 Menopause survey documenting widespread peri- and postmenopausal cannabis use for menopausal symptoms15. This is observational self-report, not clinical evidence.
- Multiple animal studies and in vitro studies linking estrogen-ECS regulation to outcomes relevant to menopausal symptoms121314. Mechanism, not clinical proof.
That is the state of the evidence as of mid-2026. There is real reason to take this seriously. There is also a clear, named gap that the field has not closed. The Rockstar Blends position is to operate honestly on top of that landscape — not to pretend the gap doesn't exist, and not to wait passively for someone else to fill it.
A second active area where I want to flag honest uncertainty is the clinical endocannabinoid deficiency framework — the proposal that some chronic conditions (migraine, fibromyalgia, IBS) reflect underlying ECS underactivity. The framework was proposed by Ethan Russo and has supporters in the field20. It is not yet broadly accepted as a clinical diagnosis. We talk about supporting the system. We do not talk about treating a deficiency.
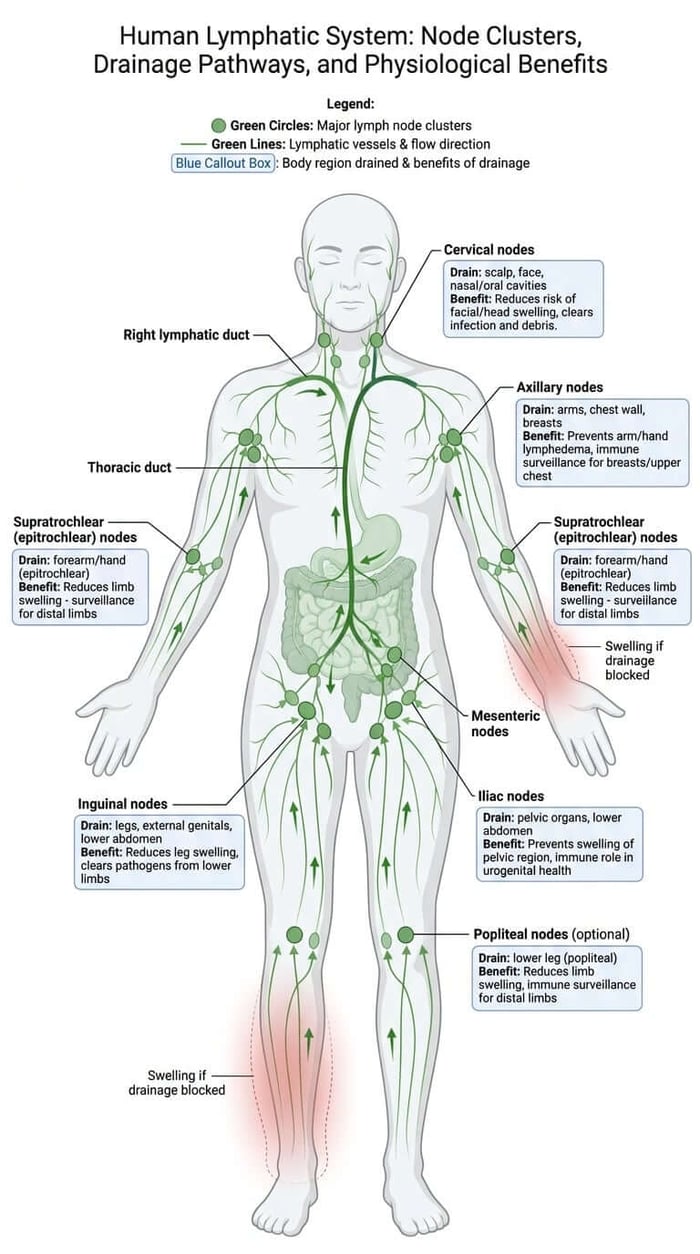
Why I do this work
When I started developing topical preparations from botanical extracts, I was thinking about my own lymphatic system and my own recovery. I was not thinking about cannabinoid receptors. The science caught up with what plant medicine practitioners had been doing for a long time, and what my doctor was teaching me to do for myself.
The reason I write posts like this one is that I want the women who come to Rockstar Blends to understand what is actually happening when they use what I make. You came here for the biology and the citations, not the tagline. You are smart, you are skeptical, you can smell hype from across the room, and you want the mechanism, the evidence, and the honest gaps. You deserve it that way.
The endocannabinoid system has been here the whole time. The science is real, it is moving fast, and the part of it that matters most for women my age is the part the menopause conversation is just beginning to catch up to.
Rockstar Woman | Natural Menopause Support
Rockstar Woman is a a topical preparation built around the receptor system described in this post; full-spectrum hemp paired with botanicals selected for their ECS-engaging compounds and formulated for our most delicate tissues.
References
- Matsuda LA, Lolait SJ, Brownstein MJ, Young AC, Bonner TI. Structure of a cannabinoid receptor and functional expression of the cloned cDNA. Nature. 1990;346(6284):561-564. Strong
- Munro S, Thomas KL, Abu-Shaar M. Molecular characterization of a peripheral receptor for cannabinoids. Nature. 1993;365(6441):61-65. Strong
- Devane WA, Hanus L, Breuer A, et al. Isolation and structure of a brain constituent that binds to the cannabinoid receptor. Science. 1992;258(5090):1946-1949. Strong
- Mechoulam R, Ben-Shabat S, Hanus L, et al. Identification of an endogenous 2-monoglyceride, present in canine gut, that binds to cannabinoid receptors. Biochem Pharmacol. 1995;50(1):83-90. Strong
- Lu HC, Mackie K. An introduction to the endogenous cannabinoid system. Biol Psychiatry. 2016;79(7):516-525. Strong
- Kano M, Ohno-Shosaku T, Hashimotodani Y, Uchigashima M, Watanabe M. Endocannabinoid-mediated control of synaptic transmission. Physiol Rev. 2009;89(1):309-380. Strong
- Pertwee RG. Cannabinoid pharmacology: the first 66 years. Br J Pharmacol. 2006;147(Suppl 1):S163-S171. Strong
- McPartland JM, Duncan M, Di Marzo V, Pertwee RG. Are cannabidiol and Δ9-tetrahydrocannabivarin negative modulators of the endocannabinoid system? A systematic review. Br J Pharmacol. 2015;172(3):737-753. Strong
- De Petrocellis L, Ligresti A, Moriello AS, et al. Effects of cannabinoids and cannabinoid-enriched Cannabis extracts on TRP channels and endocannabinoid metabolic enzymes. Br J Pharmacol. 2011;163(7):1479-1494. Strong
- Bisogno T, Hanus L, De Petrocellis L, et al. Molecular targets for cannabidiol and its synthetic analogues: effect on vanilloid VR1 receptors and on the cellular uptake and enzymatic hydrolysis of anandamide. Br J Pharmacol. 2001;134(4):845-852. Strong
- Di Marzo V. New approaches and challenges to targeting the endocannabinoid system. Nat Rev Drug Discov. 2018;17(9):623-639. Strong
- Maia J, Almada M, Silva A, et al. The endocannabinoid system expression in the female reproductive tract is modulated by estrogen. J Steroid Biochem Mol Biol. 2017;174:40-47. Moderate
- Santoro A, Mele E, Marino M, et al. The Complex Interplay between Endocannabinoid System and the Estrogen System in Central Nervous System and Periphery. Int J Mol Sci. 2021;22(2):972. Moderate
- Walker OLS, Holloway AC, Raha S. The role of the endocannabinoid system in female reproductive tissues. J Ovarian Res. 2019;12(1):3. Moderate
- Dahlgren MK, El-Abboud C, Lambros AM, et al. A survey of medical cannabis use during perimenopause and postmenopause. Menopause. 2022;29(9):1028-1036. Moderate
- Bonn-Miller MO, Feldner MT, Bynion TM, et al. A double-blind, randomized, placebo-controlled study of the safety and effects of CBN with and without CBD on sleep quality. Exp Clin Psychopharmacol. 2024;32(3):277-284. Strong
- Gertsch J, Leonti M, Raduner S, et al. Beta-caryophyllene is a dietary cannabinoid. Proc Natl Acad Sci USA. 2008;105(26):9099-9104. Strong
- Russo EB. Taming THC: potential cannabis synergy and phytocannabinoid-terpenoid entourage effects. Br J Pharmacol. 2011;163(7):1344-1364. Moderate
- Kolobaric A, Saleska J, Hewlings SJ, et al. A Randomized, Double-Blind, Placebo-Controlled Trial to Assess the Effectiveness and Safety of Melatonin and Three Formulations of Floraworks Proprietary TruCBN for Improving Sleep. Pharmaceuticals. 2024;17(8):977. Strong
- Russo EB. Clinical endocannabinoid deficiency reconsidered: current research supports the theory in migraine, fibromyalgia, irritable bowel, and other treatment-resistant syndromes. Cannabis Cannabinoid Res. 2016;1(1):154-165. Directional